Biologics are rapidly transforming modern medicine. From immunotherapies and monoclonal antibodies to mRNA vaccines and gene therapies, these complex modalities are reshaping how we treat disease and are globally expanding as a market in response.
But with that innovation comes complexity. Unlike small molecules, biologics often interact with highly specific human targets and engage intricate immune and cellular pathways. As a result, traditional development approaches, particularly those relying heavily on animal models, can face challenging translational gaps in predicting how these therapies will behave in patients. Today, the industry is reaching an inflection point as regulators and developers alike are increasingly embracing human-relevant approaches, including New Approach Methodologies (NAMs) such as microphysiological systems. The goal is not simply to replace animal testing, but to improve confidence in human outcomes and ultimately increase the clinical success rate of biologics in development.
Why biologics are uniquely challenging to develop
Biologics present a fundamentally different set of challenges compared to traditional therapeutics. Many are species-specific, meaning they interact differently with biological targets in animals. Others trigger complex immune responses that are difficult to replicate outside of a human context. As a result, animal models can be non-predictive or biologically irrelevant for certain biologics. This disconnect contributes to uncertainty in safety and efficacy and increases the risk of costly late-stage failures and wasted resources.
Regulators are increasingly acknowledging these limitations. For some biologics, particularly those without a pharmacologically relevant animal species, traditional in vivo studies may not provide meaningful insight. In these cases, alternative approaches may not only be appropriate but necessary to support development decisions.1
The opportunity for human-relevant models in biologics development
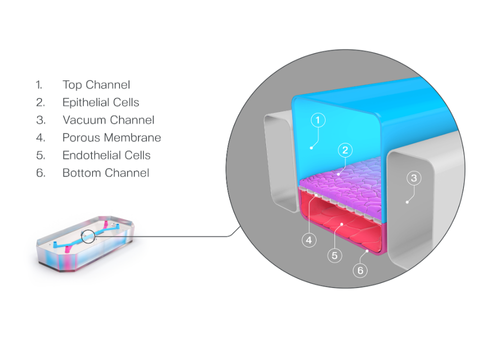
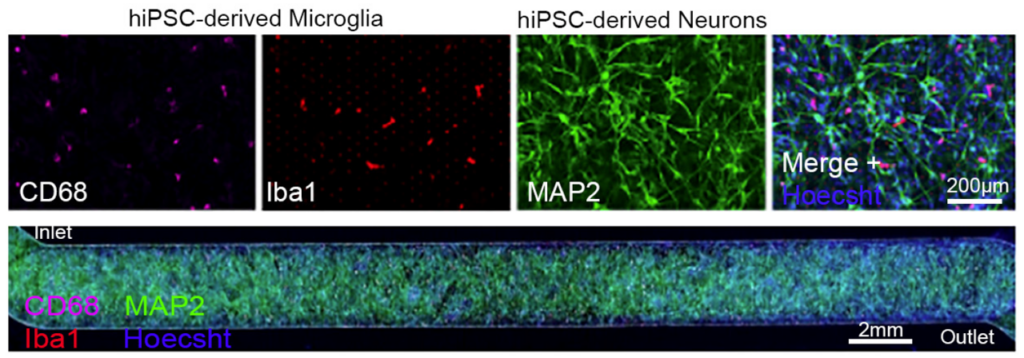
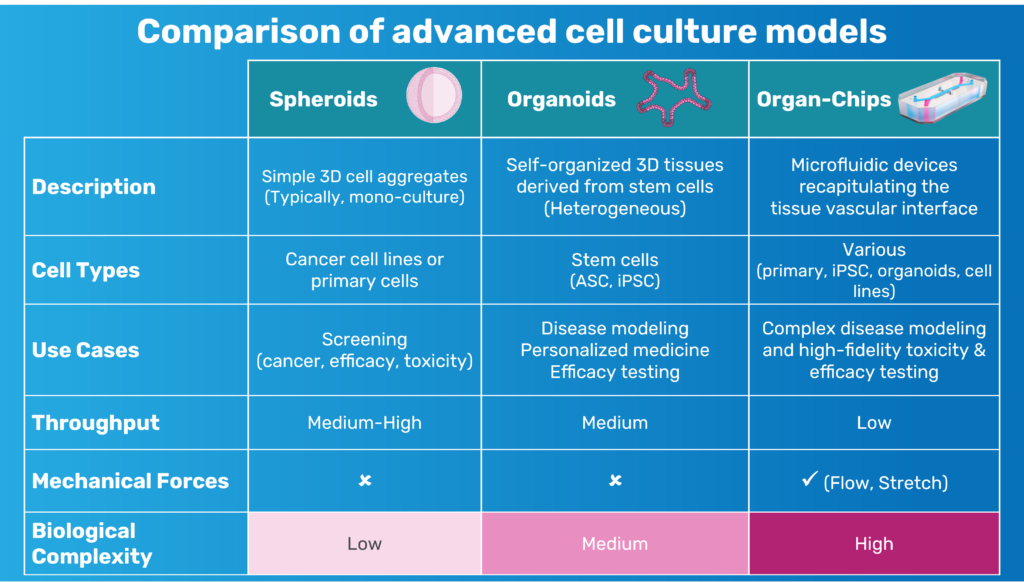
Rather than attempting to fully replace animal studies, the opportunity lies in strategically reducing reliance on them by incorporating models that better reflect human biology, such as Organ-on-a-Chip technology or other human-relevant models. These systems recreate key aspects of human tissue structure and function in a controlled, in vitro environment. By integrating multiple human cell types and simulating physiological conditions such as fluid flow, Organ-Chips enable researchers to study drug responses in a more human-relevant context.
Importantly, these systems provide more than just readouts of toxicity or efficacy. They offer critical insight into mechanisms of action, helping researchers understand how a biologic interacts with human tissues, activates immune pathways, or causes adverse effects. These insights are particularly valuable for biologics, where understanding the “why” behind a response can be just as critical as the outcome itself.2
How Organ-on-a-Chip technology fits into biologics workflows
Organ-on-a-Chip technology is not a standalone solution but is most powerful when used as part of an integrated toolkit to complement existing in vitro, in silico, and clinical data to build a more complete, human-relevant package. In biologics development, these systems are particularly valuable for addressing three common challenges: capturing mechanistic toxicology, understanding human immune behavior, and addressing common translational failures.
Mechanistic toxicology: uncovering immune-mediated risk
Immunotherapy biologics, such as T-cell bispecific antibodies (TCBs), can trigger complex immune responses that are often underpredicted in animal models. Human Organ-Chip models have been used to capture these effects in a more relevant context. For example, immunocompetent Lung- and Intestine-Chips have demonstrated target-dependent tissue damage and cytokine release, helping differentiate between higher- and lower-risk TCB designs.3 Similarly, Liver-Chip models with circulating immune cells have reproduced immune-mediated liver toxicity and linked it to specific T-cell activation pathways.4
These approaches help teams move beyond simply identifying toxicity to understanding the underlying mechanisms driving risk.
Understanding human immune behavior
For vaccines and mRNA-based biologics, development depends on understanding complex human immune responses, such as memory B-cell behavior and immune imprinting, that are difficult to study in animals. Lymphoid Organ-Chip models have enabled researchers to evaluate how different vaccine designs behave in a human immune microenvironment, including comparing booster strategies. These systems have reproduced patterns consistent with human immune imprinting, offering insight into how prior exposures shape immune responses.5
Addressing common translational failures
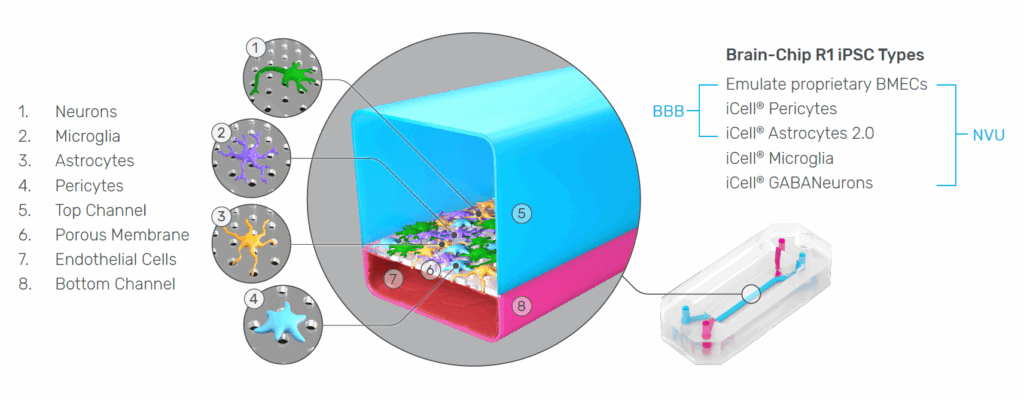
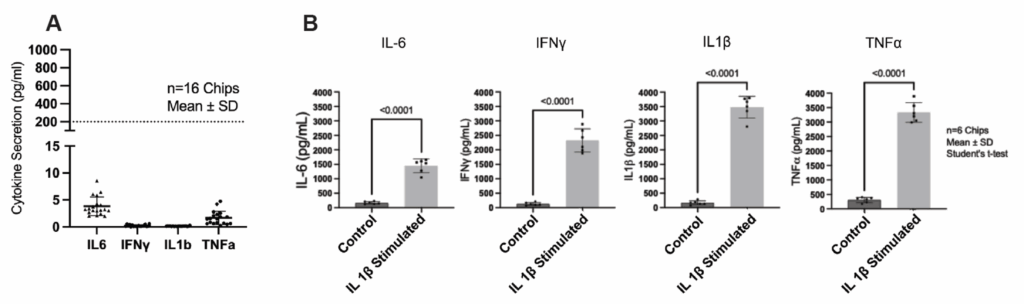
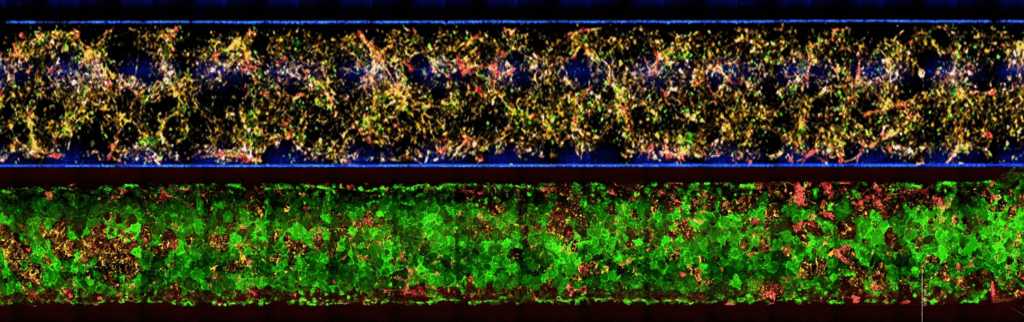
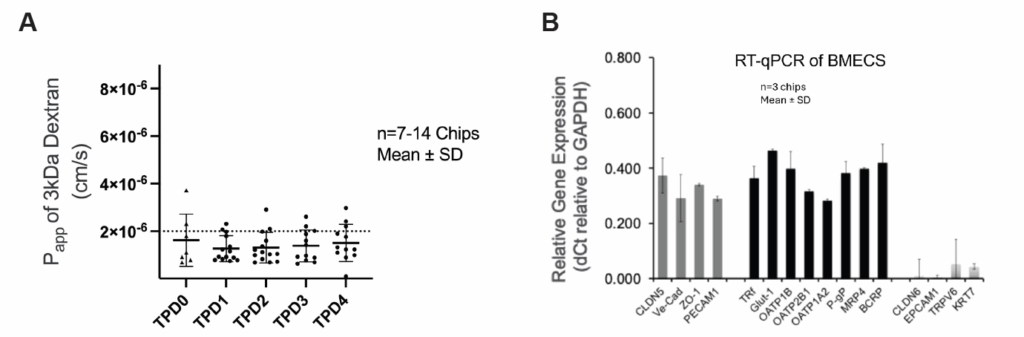
Many CNS-targeted biologics fail because they cannot effectively cross the human blood–brain barrier (BBB), a process that is difficult to predict from animal models due to species differences in transporters and receptors. Human Brain-Chips have been used to model BBB transport and neuroinflammation in a single platform. These models can differentiate between biologics based on their ability to cross the BBB, helping teams prioritize candidates earlier in development.6
Looking ahead to a more human-centric development paradigm
As scientific understanding, technology, and regulatory frameworks continue to evolve, there is growing recognition that no single model can answer every question. Instead, success will depend on selecting the right tools for the right context and integrating multiple data sources to build confidence for in-human outcomes. Organ-on-a-Chip technology plays a critical role in this shift. By enabling human-specific biology, providing mechanistic insight at the cell-type level, and demonstrating alignment with clinical outcomes, these systems can support more informed, confident decision-making. At the same time, they offer a path toward reducing reliance on exploratory animal studies, aligning with the direction of regulatory agencies and the broader push toward more ethical and predictive science.
Biologics are inherently human-specific. The models used to develop them should be as well.
Learn more
Contact Emulate to learn how Organ-Chip studies can complement or replace portions of traditional animal testing, strengthen your nonclinical strategy, and help accelerate the path to first-in-human biologics.
Watch this webinar to learn more about the current use of Emulate technology in vaccine development -> https://emulatebio.com/resources/lymphoid-organ-chip-vaccine-immunogenicity-institut-pasteur-webinar/
References
- Medicines and Healthcare products Regulatory Agency. (2026, March 25). MHRA approach to medicines using non-animal methods. GOV.UK. https://www.gov.uk/guidance/mhra-approach-to-medicines-using-non-animal-methods
- Armstrong, R. (2026, March 30). The opportunities and challenges for antibody-based therapies. Drug Discovery World. https://www.ddw-online.com/the-opportunities-challenges-for-antibody-based-therapies-41097-202603/
- Kerns, S. J., Belgur, C., Petropolis, D. et al. (2021). Human immunocompetent Organ-on-Chip platforms allow safety profiling of tumor-targeted T-cell bispecific antibodies. eLife, 10, e67106. https://doi.org/10.7554/eLife.67106
- Chaff, J. et al. (2024). Evaluating the immunotoxicity of CD137-induced agonism on the Emulate Human Liver-Chip. Emulate, Inc. https://emulatebio.com/resources/evaluating-immunotoxicity-of-cd137-induced-agonism-on-emulate-human-liver-chip-poster-sot-2024/
- Jeger-Madiot, R. et al. (2024). Modeling memory B cell responses in a lymphoid organ-chip to evaluate mRNA vaccine boosting. The Journal of experimental medicine, 221(10), e20240289. https://doi.org/10.1084/jem.20240289
- Chim, S. M., Howell, K., Kokkosis, A., Zambrowicz, B., Karalis, K., & Pavlopoulos, E. (2024). A Human Brain-Chip for Modeling Brain Pathologies and Screening Blood–Brain Barrier Crossing Therapeutic Strategies. Pharmaceutics, 16(10), 1314. https://doi.org/10.3390/pharmaceutics16101314