What is Gene Therapy?
Gene therapy is the modification, manipulation, or deletion of genes to treat, prevent, or cure a disease. Often used in diseases or disorders thought to be incurable by conventional modalities, gene therapy can be life changing for patients.1
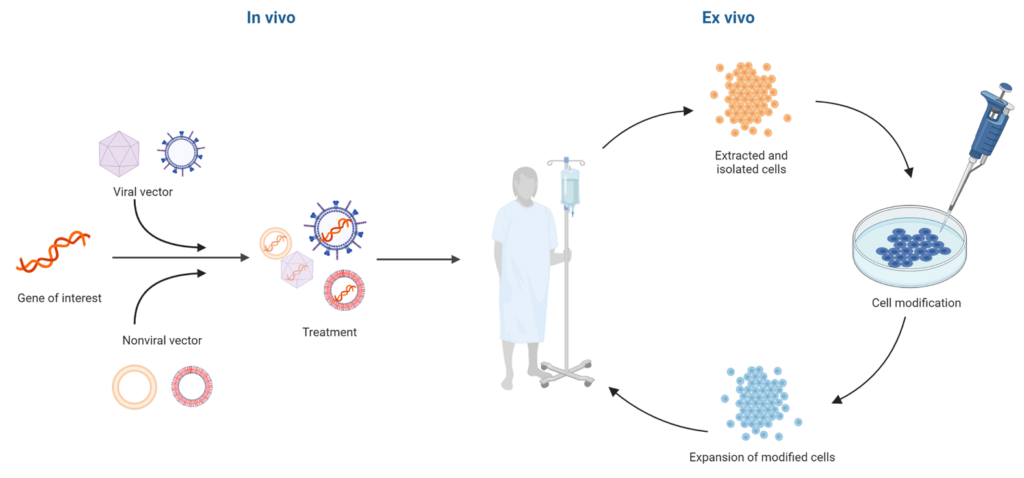
Figure 1. The basic gene therapy process
There are two types of gene therapy: in vivo and ex vivo. Briefly, in vivo gene therapy is administered directly by packaging a gene of interest into a viral or nonviral vector and injecting the treatment into the patient (Figure 1, left). In contrast, ex vivo gene therapy is administered to cells that have been extracted from the patient. These extracted cells are genetically modified in culture, grown, expanded, and then infused back into the patient (Figure 1, right).2
Stay Up to Date with Emulate
A Brief History of Gene Therapy
Gene therapy began nearly 80 years ago, when Clyde E. Keeler conceptualized the practice of correcting genes in plants and animals.3 Research into gene therapy steadily increased throughout the 1960s and 1970s; by 1999, there were over 2000 clinical trials (Figure 2).3 However, all progress would soon come to a halt.
Jesse Gelsinger, a teenager from Arizona, had been born in 1981 with a condition that caused ammonia to build up in the blood. Using early gene therapy methods, doctors had successfully extended the lives of mice with the same condition; in 1999, Jesse enrolled in the one of the first clinical trials to see if the effect could be replicated in humans. Unfortunately, the results were not as intended. Jesse’s health quickly deteriorated, and he ultimately passed away.4 The death of Jesse Gelsinger caused all trials in the US to come to an abrupt pause.
Despite the setbacks from that tragic event, the field eventually rebounded. Today, there are 27 cell and gene therapy products approved by the Food and Drug Administration (FDA) and over 1200 gene therapy trials registered with ClinicalTrials.gov that are actively recruiting.
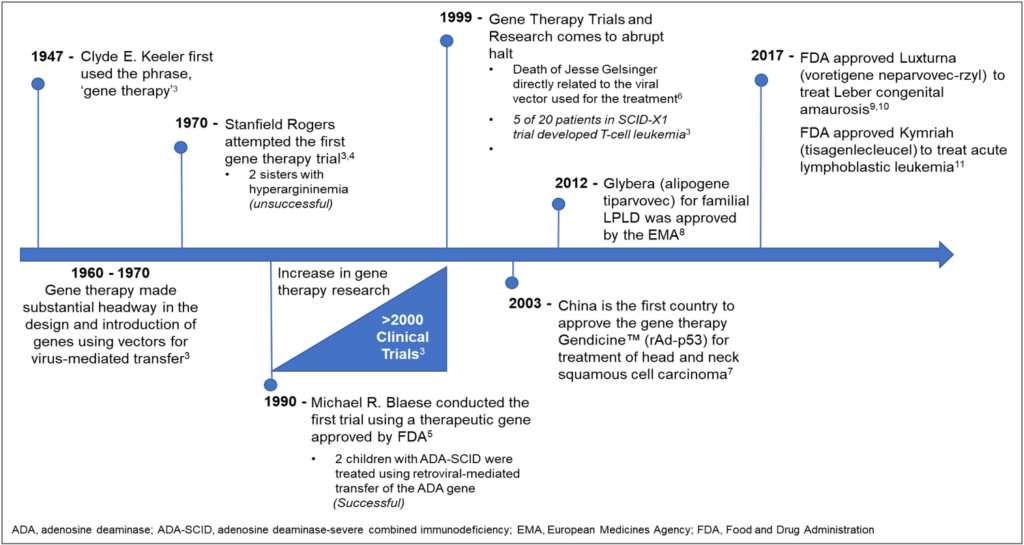
Figure 2. History of Gene Therapy3, 5-12
Examples of Gene Therapy
While gene therapy has applications across a wide variety of diseases, it has been particularly useful in researching cancer treatments, as many types of human cancer develop through genetic alterations. In fact, over 65% of the global gene therapy clinical trials are cancer-related2, with several receiving FDA approval in recent years. For example, Kymriah (tisagenlecleucel), the first gene therapy that is FDA-approved for medical use, is a chimeric antigen receptor (CAR) T cell genetic therapy for treating acute lymphoblastic leukemia (ALL), one of the most common pediatric and young adult cancers.13 Clinical trial data showed that 56% of all patients achieved sustained remission following treatment with Kymriah.
Breast cancer is another area that stands to benefit greatly from targeted gene therapies. Of the inherited forms of breast cancer, the most common cause is mutations in BRCA1 and BRCA2 genes.14 Gene therapy could help prevent inherited breast cancer by replacing the mutated version of these genes with functional versions. For non-inherited forms of breast cancer, gene therapy can be used to target oncolytic genes that drive cancer progression. According to ClinicalTrials.gov, many gene therapy trials are actively recruiting patients, with several showing promising results.
Another major area gene therapy could benefit is research into rare diseases. While thousands of rare diseases have been identified, only a small percentage have approved treatments. As more than 80% of rare diseases can be attributed to mutations in a single gene, gene therapy offers the potential to correct the underlying disease instead of minimizing symptoms with traditional treatments.15 For example, the gene therapies under development for cystic fibrosis (CF) aim to deliver a functional copy of the cystic fibrosis transmembrane conductance regulator (CFTR) gene into the lung, replace the mutated version of the protein, and permanently reduce CF symptoms in the lungs.
Other applications of gene therapy include:
- Neuromuscular and central nervous system disorders, such as Huntington’s and Parkinson’s disease
- Blood disorders, such as hemophilia and β-thalassemia
- Ocular disorders
- Diabetes
- Osteoarthritis
- Cardiac arrhythmias
- Hearing and balance disorders16-19
Additionally, recent successes in gene therapy could lead to treatments for several diseases and disorders (Table 1).
| Recent Milestones in Gene Therapy | ||
| 2021 | 1. Experimental gene therapy reverses sickle cell in patients for up to 37.6 months20 2. Inherited gene mutation is disabled in transthyretin (TTR) amyloidosis, directly through an infusion of the genome editor CRISPR21 3. The first-in-human Phase I clinical trial begins for gene therapy to assess the safety and efficacy in Alzheimer’s disease or Mild Cognitive Impairment22 | FDA Approvals ABECMA—cell-based gene therapy for multiple myeloma BREYANZI—cell-based gene therapy large B-cell lymphoma (LBCL) RETHYMIC—tissue-based therapy for congenital athymia STRATAGRAFT—tissue-based therapy for thermal burns |
| 2022 | 1. Trials in the US and Europe with a hemophilia B gene therapy called FLT180a (verbrinacogene setparvovec) using a synthetic AAV vector shows that 90% of trial participants still did not need regular injections after 2 years23 2. Two of the earliest CAR T cell therapy patients with cancer had survived over ten years post therapy24 3. Early preclinical success in injectable cell and gene therapy for prostate cancer, liver cancer, and leukemia24 | FDA Approvals ADSTILADRIN—gene-based therapy for non-muscle invasive bladder cancer (NMIBC) with carcinoma in situ (CIS) CARVYKTI—cell-based therapy for multiple myeloma HEMGENIX—gene-based therapy for hemophilia B SKYSONA—gene-based therapy to slow the progression of early, active cerebral adrenoleukodystrophy (CALD) ZYNTEGLO—gene-based therapy for ß-thalassemia |
Advantages and Disadvantages of Gene Therapy
Gene therapy, as with many new types of treatment, comes with many potential benefits as well as some risks and safety concerns (Table 2). These pros and cons must be balanced if researchers want to create a therapy that is safe, effective, and commercially viable.
As discussed above, gene therapy has numerous advantages over conventional disease treatments. By replacing defective genes, gene therapy has the ability to correct underlying disease mechanisms instead of just treating symptoms, with significantly less dosing frequency. In fact, some gene therapies could cure diseases in as few as one treatment. Gene therapy is also a versatile tool, with the ability to target a multitude of genes across various diseases.
However, gene therapy brings several potential risks. While the most common adverse side effect of gene therapy is liver toxicity, others include moderate to severe immune responses, development of certain types of cancer, and damage to organs or tissues. Poor outcomes have been largely traced back to the challenges surrounding the vectors, which are the vehicles that delivers therapeutic genetic material to cells. As such, researchers have focused on improving gene delivery technologies, which has led to safer viral and non-viral vectors, standardized production processes, and refined clinical protocols with better patient screening and dosing strategies. Collectively, these modifications have significantly improved the safety of gene therapy since the first clinical trials in the 1970s.
| Advantages of gene therapy | Disadvantages of gene therapy |
| 1. Versatile tool that can be applied to treat, prevent, or cure complex diseases, including vision loss, cancer, blood disorders, and spinal muscular atrophy. 2. Often individualized, increasing the possibility of success. 3. Could cure diseases with as little as one treatment. | 1. Efficacy of therapy with AAV vectors are dose dependent, and higher doses may cause adverse events.26 2. Safety concerns due to gene integration 3. Certain treatments are not permanent and would need to be re-administered to maintain effectiveness. 4. Can be expensive25; in the US, costs can range from $373,000 to $2.1M per treatment. |
Gene Therapy Development Process
Bringing a gene therapy to market can be complex, costly, and time consuming. One of the most challenging aspects of gene therapy is developing vectors that are safe and effective. The most important criteria in designing an effective vector are protection for the genetic cargo, delivery to the target site, minimal immunogenicity and genotoxicity, and cost-effective patient access.27
There are multiple types of vectors that can be used, but they are generally classified as either viral or non-viral. Each type of vector is associated with risks. Thus, it is critical to rigorously test vectors in preclinical development and identify any toxicities or negative side effects they could cause.
Viral vectors commonly include adenoviruses (Ads) and adeno-associated viruses (AAVs). Adenoviruses were first used as vectors approximately 20 years ago and have many advantages, such as a broad range of tissue tropism, high transduction efficiency, and a well-characterized genome. They typically exhibit low pathogenicity and toxicity and can provide long-term transgene expression. However, repeated exposure can increase adverse immune responses.27 These challenges can be overcome by using different adeno-associated viral (AAV) serotypes to reduce immunogenicity. Other types of viral vectors include retroviruses, lentiviruses, poxviruses, and vaccinia viruses, which are less commonly used due to complexity of viral structure, safety concerns, and genotoxicity, although lentivirus has had success ex vivo in CAR T cell therapies.28,29
Non-viral vectors are made from a variety of materials, including polymers, lipid nanoparticles (LNPs), inorganic materials (e.g., gold nanoparticles and carbon nanotubes), and hybrid systems (e.g., peptide-lipid vectors).30 Compared to their viral counterparts, non-viral vectors have lower immunogenicity and cytotoxicity and can handle a larger payload.30,31 However, non-viral vectors typically exhibit low transduction efficiency, and some can illicit an immune response, which requires evaluation with each new vector created. Other challenges are physical and chemical stability, consistency of a vector during formulation preparation as well as product storage, and vector-system complexities. However, ongoing research seeks to optimize non-viral vectors for use in gene therapies, such as the recent LNP-based gene therapy for Stargardt disease.32 Non-viral vectors have also been successfully used for applications outside of gene therapy, such as with the two mRNA coronavirus-19 (COVID-19) vaccines produced by Moderna and Pfizer-BioNTech, which use LNPs as the vector for mRNA delivery.
Given that only a few gene therapies have reached the market despite decades of research, there are clearly hurdles this type of treatment must overcome on the road to widespread use. Gene therapy candidates frequently fail in clinical trials due to severe adverse events that were not predicted by the experiments performed on in vitro and in vivo models prior to clinical trials. Current preclinical in vivo models present challenges in that they poorly predict human drug responses, safety, and efficacy. This is on top of the ethical concerns that using animal experimentation brings.33 Meanwhile, conventional in vitro models lack the complexity to fully emulate human physiology, lacking critical features such as 3D cytoarchitecture, cell-cell interactions, and cell heterogeneity34. Thus, there is a great unmet need for suitable preclinical models that can provide adequate clinical translation.
Organ-Chips for Gene Therapy
Researchers can use Organ-on-a-Chip technology to circumvent the challenges of traditional preclinical models in gene therapy by better predicting possible safety concerns, evaluating transduction efficiency, assessing immune response, and avoiding species translation issues.
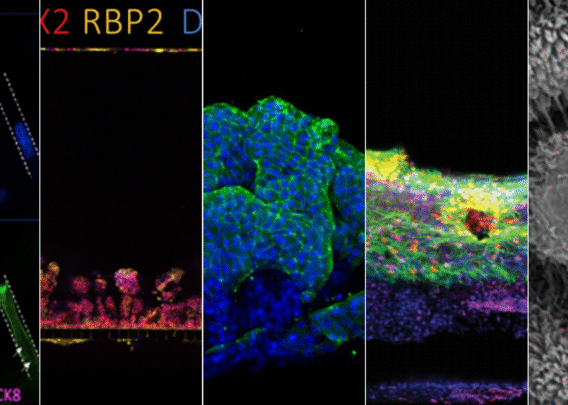
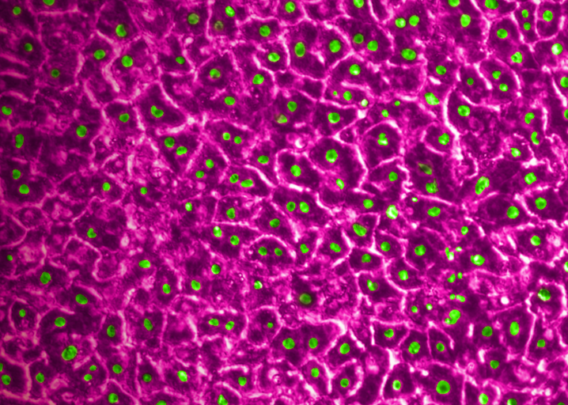
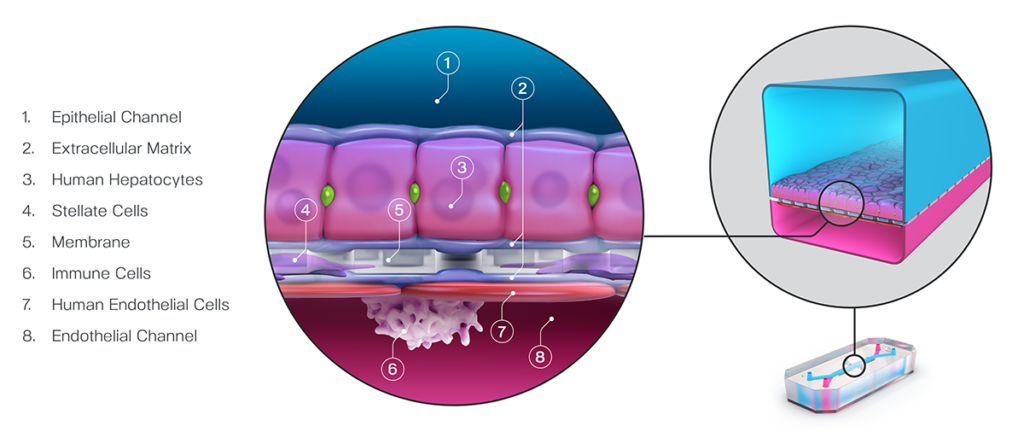
Take for example the Emulate human Liver-Chip’s ability to improve AAV-based gene therapy development. The liver is a target of many gene therapies due to its important role in several essential biological processes. However, hepatotoxicity is a major obstacle in bringing gene therapies to the clinic. Improved preclinical liver models could reduce human toxicity, patient adverse events, clinical attrition, and overall failure rates of gene therapy candidates. The Liver-Chip from Emulate is a physiologically relevant model of the human liver that incorporates all key hepatic cell types in the sinusoid (Figure 3).35 It can be used to generate human-relevant data in weeks, as opposed to the months it would take with animal models, which can decrease development timelines and facilitate rapid iteration in designing therapy vectors.
Testing AAVs, including AAV2 and AAV6 vectors, on the Liver-Chip showed that it could reliably measure concentration-, time-, and serotype-dependent transduction for 7 days. Toxic responses could be confirmed through performing common functional liver endpoint assays such as testing albumin and alanine transaminase (ALT) levels.
In a proof-of-concept study, a proprietary AAV construct was administered to the chip’s endothelial channel to mimic the intravenous administration route (Figure 4). After 7 days, AAV vector transport across the endothelial channel to the epithelial tissue could be measured in a distinct dose-dependent hepatocyte transduction. This would enable researchers to assess a vector’s tropism through a clinically relevant route of administration.
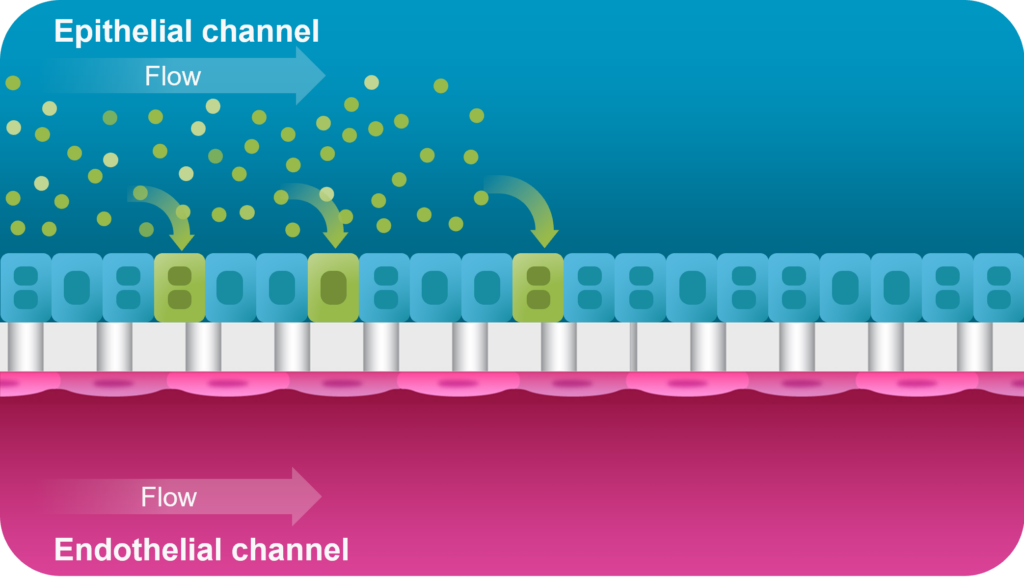
The data supports the use of Organ-Chips for testing AAV-based gene therapies to model intravenous treatments, assess transduction efficiency, and measure relevant clinical biomarkers to monitor for signals of hepatotoxicity. In addition, mechanisms of vector targeting can be further analyzed to provide insights for new vector designs. Better understanding of the biology of viral vectors and their interactions within the body can lead to improved clinical trials for different indications.
Taken together, gene therapy is rapidly evolving with the promise of improving treatment strategies for many genetic and inherited diseases that currently have no cure. While there are several challenges in gene therapy development, Organ-on-a-Chip technology provides a solution to improve the poor species translation that impedes current preclinical models. As such, Organ-Chips offer a platform for better predicting the benefits, safety, risks, and overall success of gene therapies in humans.
References
- Bulaklak, K. & Gersbach, C. A. The once and future gene therapy. Nat. Commun. 11, (2020).
- Belete, T. M. The current status of gene therapy for the treatment of cancer. Biol. Targets Ther. 15, 67–77 (2021).
- Braun, S. History of Gene Therapy. in Advanced Textbook On Gene Transfer, Gene Therapy And Genetic Pharmacology: Principles, Delivery And Pharmacological And Biomedical Applications Of Nucleotide-based Therapies (ed. Scherman, D.) 17–29 (World Scientific, 2019). doi:10.1142/Q0205#t=suppl.
- Rinde, Meir. “The Death of Jesse Gelsinger, 20 Years Later.” Science History Institute, Science History Institute, 4 June 2019, www.sciencehistory.org/distillations/the-death-of-jesse-gelsinger-20-years-later.
- Terheggen, H. G., Lowenthal, A., Lavinha, F., Colombo, J. P. & Rogers, S. Unsuccessful trial of gene replacement in arginase deficiency. Eur. J. Pediatr. 1975 1191 119, 1–3 (1975).
- Blaese, R. M. et al. T Lymphocyte-Directed Gene Therapy for ADA− SCID: Initial Trial Results After 4 Years. Science (80-. ). 270, 475–480 (1995).
- Stolberg, S. G. The biotech death of Jesse Gelsinger. The New York times magazine 136-140,149-150 (1999).
- Wilson, J. M. Gendicine: the first commercial gene therapy product. Human gene therapy vol. 16 1014–1015 at https://doi.org/10.1089/hum.2005.16.1014 (2005).
- European Medicines Agency recommends first gene therapy for approval | European Medicines Agency. https://www.ema.europa.eu/en/news/european-medicines-agency-recommends-first-gene-therapy-approval.
- Padhy, S. K., Takkar, B., Narayanan, R., Venkatesh, P. & Jalali, S. Voretigene neparvovec and gene therapy for leber’s congenital amaurosis: Review of evidence to date. Appl. Clin. Genet. 13, 179–208 (2020).
- FDA approves novel gene therapy to treat patients with a rare form of inherited vision loss | FDA. https://www.fda.gov/news-events/press-announcements/fda-approves-novel-gene-therapy-treat-patients-rare-form-inherited-vision-loss.
- FDA approval brings first gene therapy to the United States | FDA. https://www.fda.gov/news-events/press-announcements/fda-approval-brings-first-gene-therapy-united-states.
- Daley, J. Four Success Stories in Gene Therapy. Nature (2021) doi:10.1038/D41586-021-02737-7.
- Lima, Z. S. et al. Recent advances of therapeutic targets based on the molecular signature in breast cancer: genetic mutations and implications for current treatment paradigms. J. Hematol. Oncol. 12, 38 (2019).
- Brook PJ, Yang NN, Austin CP. Gene therapy: the view from NCATS. Hum Gene Ther. 27 (1), 7-13 (2016).
- Dastjerd, N. T. et al. Gene therapy: A promising approach for breast cancer treatment. Cell Biochem. Funct. 40, 28–48 (2022).
- Shahryari, A., Burtscher, I., Nazari, Z. & Lickert, H. Engineering Gene Therapy: Advances and Barriers. Adv. Ther. 4, 2100040 (2021).
- Mendell, J. R. et al. Current Clinical Applications of In Vivo Gene Therapy with AAVs. Mol. Ther. 29, 464–488 (2021).
- Arabi, F., Mansouri, V. & Ahmadbeigi, N. Gene therapy clinical trials, where do we go? An overview. Biomed. Pharmacother. 153, 113324 (2022).
- Kanter, J. et al. Biologic and Clinical Efficacy of LentiGlobin for Sickle Cell Disease. N. Engl. J. Med. 386, 617–628 (2022).
- First gene-editing treatment injected into the blood reduces toxic protein for up to 1 year | Science | AAAS. https://www.science.org/content/article/first-gene-editing-treatment-injected-blood-reduces-toxic-protein-1-year.
- First-in-Human Clinical Trial to Assess Gene Therapy for Alzheimer’s Disease. https://health.ucsd.edu/news/press-releases/2021-02-18-first-in-human-clinical-trial-to-assess-gene-therapy-for-alzheimers-disease/.
- Chowdary, P. et al. Phase 1–2 Trial of AAVS3 Gene Therapy in Patients with Hemophilia B. N. Engl. J. Med. 387, 237–247 (2022).
- Top Stories for Cancer Cell and Gene Therapy in 2022 | Alliance for Cancer Gene Therapy. https://acgtfoundation.org/news/top-stories-cancer-cell-and-gene-therapy-2022/.
- Mercier, J., Ruffin, M., Corvol, H. & Guillot, L. Gene Therapy: A Possible Alternative to CFTR Modulators? Front. Pharmacol. 12, 505 (2021).
- Moutsatsou, P., Ochs, J., Schmitt, R. H., Hewitt, C. J. & Hanga, M. P. Automation in cell and gene therapy manufacturing: from past to future. Biotechnol. Lett. 41, 1245–1253 (2019).
- Butt, M. H. et al. Appraisal for the Potential of Viral and Nonviral Vectors in Gene Therapy: A Review. Genes 2022, Vol. 13, Page 1370 13, 1370 (2022).
- Lundstrom, K. Viral Vectors in Gene Therapy. Diseases 6, 42 (2018).
- Bulcha, J. T., Wang, Y., Ma, H., Tai, P. W. L. & Gao, G. Viral vector platforms within the gene therapy landscape. Signal Transduct. Target. Ther. 2021 61 6, 1–24 (2021).
- Zu, H. & Gao, D. Non-viral Vectors in Gene Therapy: Recent Development, Challenges, and Prospects. AAPS J. 23, 1–12 (2021).
- Ramamoorth, M. & Narvekar, A. Non Viral Vectors in Gene Therapy- An Overview. J. Clin. Diagn. Res. 9, GE01 (2015).
- Sun, Da, et al. Effective Gene Therapy of Stargardt Disease with PEG-ECO/PGRK1-ABCA4-S/MAR Nanoparticles. Vol. 29, 1 Sept. 2022, pp. 823–835, https://doi.org/10.1016/j.omtn.2022.08.026. Accessed 27 July 2023.
- Li, C. & Samulski, R. J. Engineering adeno-associated virus vectors for gene therapy. Nat. Rev. Genet. 2020 214 21, 255–272 (2020).
- Choi, S. H. & Engelhardt, J. F. Gene Therapy for Cystic Fibrosis: Lessons Learned and Paths Forward. Mol. Ther. 29, 428–430 (2021).
- Jang, K. J. et al. Reproducing human and cross-species drug toxicities using a Liver-Chip. Sci. Transl. Med. 11, (2019).